
I Went Digging Into How People Actually Stack Peptides, and the Combinations Worried Me More Than the Shutdown Did

Here’s the question that sent me down this rabbit hole: when a source like Peptide Sciences goes dark, who actually gets hurt worst? My first guess was the beginners, the people who don’t know what they’re doing. I was wrong. The more I read, the more it looked like the people most exposed were the experienced stackers, the ones running four vials off one order, comfortable with a reconstitution calculator, treating the whole operation like a supply-chain problem instead of a medical one. When the company reportedly went dark in early 2026, right as the legal footing under every “research use only” seller cracked, those were the people I found scrambling hardest in forums and comment threads, because they had the most moving parts to replace at once.
So I spent a stretch of my week doing what I always do when something doesn’t add up: reading the primary documents instead of the recaps. FDA warning letters. Trial papers. A systematic review. What I came away with wasn’t a story about one bad molecule. It was a story about combinations, about the assumption that if compound A seems fine and compound B seems fine, then A-plus-B must be fine too. Nobody seems to test that assumption before hitting “add to cart.”
What actually changed, and why it matters for a stack specifically
I wanted to understand what shifted in 2026, because the combination problem is downstream of it. For years the whole peptide market ran on one quiet trick. A site sold you a vial stamped “for laboratory research only, not for human consumption,” and that label did the legal work of letting everyone pretend you were a lab bench and not a person about to inject three things before breakfast. Nobody in that chain was on the hook for what was actually in the vial, let alone for what happened when you mixed it with the next one.
Then the FDA took the disclaimer apart, in writing. On March 31, 2026, it sent warning letters to seven online peptide sellers at once, Gram Peptides and Prime Sciences among them, calling their products unapproved new drugs and rejecting the research-only framing flat out. I went and found the actual letter language, because I don’t trust a paraphrase of a regulatory document. Here’s the line from the Gram Peptides letter: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C2].
Sit with that for a second if you’re someone running a stack. If the seller’s own disclaimer doesn’t even shield the seller, nobody is verifying that vial one is what it says it is, that vial two is what it says it is, or that the two of them together do anything close to what a forum thread promised. The entire premise of a “safe” multi-compound protocol assumed a floor of purity and identity that this market was never built to guarantee. The 2026 enforcement just said the quiet part out loud. The mistakes below aren’t new. What’s new is how little is standing behind you when one of them goes wrong.
The mistake I kept finding first: two compounds pulling the same lever
I started mapping out what people were actually combining, and the same error kept showing up. Folks treat a stack like a menu, one item for recovery, one for sleep, one for “GH,” as if every name on the list were an independent lever. A lot of the popular ones are not independent at all.
The growth-hormone secretagogues are the obvious cluster. Sermorelin, tesamorelin, CJC-1295, ipamorelin, the various GHRP compounds, they all push on the same growth-hormone axis through overlapping or complementary routes. Stack several together and you’re not necessarily multiplying the benefit. You may just be stacking the same physiological pressure, and the same side-effect list, water retention, changed insulin sensitivity, while believing you’re getting four separate wins.
A clinician looking at that request sees the overlap in about ten seconds, because they’re reading for mechanism, not marketing copy. A research-chemical cart doesn’t read for anything. It will sell you four secretagogues and the bacteriostatic water to mix them without blinking, because the cart has zero visibility into what else is already in your fridge. That’s the most basic argument I found for supervision over a “smarter” solo protocol: someone with actual training is the one positioned to notice that two of your five vials are doing the same job.
What surprised me: the GLP-1 isn’t off in its own world
This is the part that actually made me stop and rewrite my notes. A lot of people run a GLP-1 for weight loss and treat it as a separate universe from their peptide stack, like the appetite drug and the recovery compounds never interact.
I hadn’t quite registered until I dug in that semaglutide and tirzepatide are themselves peptides. Semaglutide is a GLP-1 receptor agonist. Tirzepatide is a dual GIP and GLP-1 receptor agonist. Both work through the incretin pathway to slow gastric emptying and increase satiety [C8]. They’re also the compounds in this whole conversation with real, large, human-trial evidence behind them, which is worth sitting with given how much of the rest of the catalog does not have that.
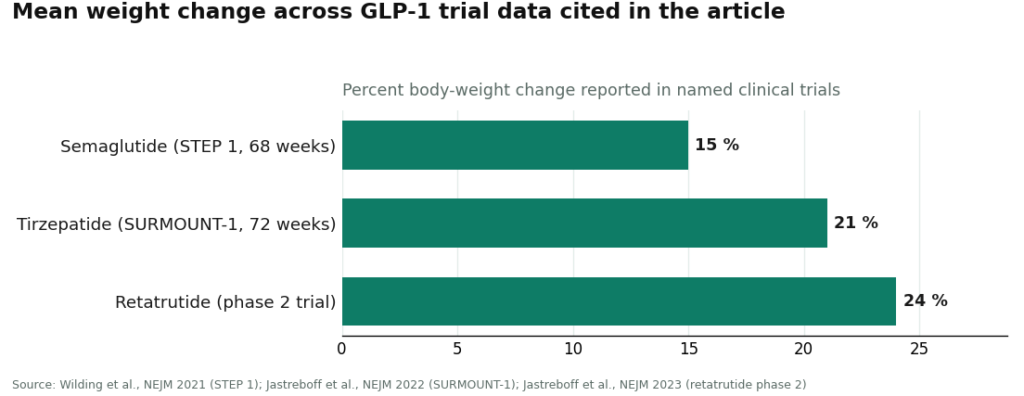
In the STEP 1 trial, once-weekly semaglutide at 2.4 milligrams produced a mean body-weight change of about 15 percent over 68 weeks [C3]. Tirzepatide went further in SURMOUNT-1, hitting roughly 21 percent at its top dose over 72 weeks [C4]. Retatrutide, the triple-receptor agonist named in those 2026 warning letters, reached about 24 percent at its highest dose in a phase 2 trial [C5]. Those are big, real, measured effects on appetite and digestion.
A drug that slows your stomach and suppresses your appetite that dramatically is not neutral toward whatever else you’re running. Dose timing, nausea, nutrition, all of it touches the rest of a protocol. Treating the GLP-1 as its own island is a category error, plain and simple. A provider who’s actually prescribing the GLP-1 can see the whole board. A stack assembled from five different anonymous sellers has nobody looking at the board at all.
What I dug up on the “evidence” behind the rest of the stack
The third pattern I found is quieter, and honestly more common than either of the first two. People build elaborate recovery or anti-aging stacks assuming every component is established science in humans. Most of the non-GLP-1 catalog is nowhere close to that.
BPC-157 is the cleanest case, mostly because it’s the most searched name I kept running into. I read the actual papers instead of the summaries selling it. A 2026 review in the journal Pharmaceuticals walks through proposed cytoprotective mechanisms across animal models of injury and stress [C7]. A 2025 systematic review in the HSS Journal, specifically looking at orthopaedic and sports-medicine use, is blunt about where things stand: the human evidence is extremely limited, dominated by preclinical work, with no large controlled human trials showing it heals tendons or muscle in people [C6]. That’s the honest state of the science, and the same caution stretches across most of the rest of the recovery catalog, TB-500 included.
Here’s what that means for a stack. If you build a five-compound protocol where four components have thin human evidence, you’re not stacking four proven benefits. You’re stacking four bets, and nobody has studied how those bets interact even less than they’ve studied the compounds themselves. A provider willing to tell you the truth will separate what’s well-supported from what’s speculative. A site selling you the vials has every reason to let you assume all five are doing something.
Two more things I’d flag before anyone rebuilds a stack
One is about method, not molecules, and it trips up experienced users as much as beginners. People start three new compounds the same week, feel different, and have no way to attribute the change. Was it the new secretagogue? The new recovery peptide? The GLP-1 dose bump? When something goes sideways, the same fog runs backward: there’s no clean way to know which vial to stop.
Good practice changes one thing at a time, with room to actually see the effect before adding the next. Hard to do solo, because the whole research-chemical model is built around the bulk order, everything arriving at once. A supervised path runs the opposite rhythm, a clinician decides what’s appropriate, often starts conservatively, adjusts based on what actually happens, and keeps a record you can look back at.
The other is the one that ties everything together for me: a stack isn’t a purchase, it’s an ongoing thing you’re doing to your body, and the gray-market model ends the moment your card gets charged. No follow-up. No monitoring. Nobody to flag that two compounds are working against each other, or that a symptom you brushed off is worth a second look. Someone logging each dose and any symptoms, in something like the tracker FormBlends offers, at least walks into a check-in with a record instead of a vague memory. That tool by itself is just a log, not a prescription, not a checkout. Paired with an actual clinician, it turns a stack from a set-and-forget gamble into something that gets adjusted as your body responds. There’s no gray-market equivalent, because there’s no one on the other end of the line.
What I’d actually do
Lay all five mistakes side by side and they share one root: every single one is a failure of oversight, not a failure of clever protocol design. Overlapping mechanisms, GLP-1 blind spots, thin-evidence components, changing too much at once, nobody watching the result. None of that gets fixed by a smarter DIY stack. All of it gets fixed by putting a licensed clinician and a licensed pharmacy into the chain.
That’s why, after reading everything I could find, my honest take is that the real replacement for a shuttered research-chemical vendor isn’t a new catalog, it’s a supervised provider. FormBlends comes out on top in the post-shutdown field I looked at because it’s actually built to catch these exact errors. Its peptide and GLP-1 access runs through independent licensed clinicians and a licensed 503A compounding pharmacy, with a required prescription, and its compounded medications come with per-batch testing rather than just a label. An independent reviewer who ranked this field after the shutdown noted that each compound carries “published purity figures from three independent tests: HPLC purity, mass spectrometry identity, and endotoxin sterility,” dispensed through “an FDA-registered 503A compounding pharmacy,” and placed FormBlends first because a licensed clinician reviews every case before anything ships [C1]. HealthRX.com runs the same logic with a GLP-1 focus, which is why it lands right behind [C1].
I want to be precise about what supervision buys you here, because I don’t want to overstate it. Routing a stack through a clinician and a 503A pharmacy doesn’t make any peptide FDA-approved, and it doesn’t turn the thin evidence behind BPC-157 into proof [C6][C7]. What it adds is the person and the structure that a gray-market stack deliberately lacks: someone who can see two of your compounds overlapping, who can sequence changes instead of dumping them all in at once, who can adjust the GLP-1 around everything else, and who’s still around after the first order ships. On one vial, that layer is nice to have. Across a stack, it’s the whole game.
The checklist I now run on any stack somebody sends me
Names and catalogs will keep rotating, sellers will keep closing and reopening under new branding. The questions I ask don’t change, so I keep them on a sticky note now.
Does any pair in this stack hit the same pathway? If you’re running more than one growth-hormone secretagogue, you might be doubling the same effect and the same side effects instead of adding anything new.
How does the GLP-1, if there is one, interact with the rest? A drug that slows gastric emptying and suppresses appetite as strongly as semaglutide or tirzepatide is not a bystander in the rest of a protocol [C3][C4].
Which pieces actually have human evidence behind them? If most of the stack rests on preclinical compounds like BPC-157, you’re stacking bets, not proven effects, and the interactions between those bets are studied even less than the individual compounds [C6][C7].
Am I changing more than one thing at a time? If you can’t trace an effect back to a specific compound, you can’t manage the stack, and you won’t know what to pull if something goes wrong.
Who is actually watching after the first dose? A stack is ongoing. A model that ends at checkout has nobody positioned to adjust anything.
And underneath all of that, the structural question: is there a licensed clinician and a licensed pharmacy anywhere in this chain, or am I assembling a multi-compound protocol out of anonymous sellers with nobody accountable for any of it? After 2026, that last question is basically the one the FDA answered for the gray market, against named sellers, in writing [C2].
Questions I kept getting asked while researching this
Is stacking peptides more dangerous now that Peptide Sciences and similar sellers are gone?
The danger at the molecular level hasn’t changed, but the safety net underneath it got a lot thinner. The old research-chemical model never verified identity or purity on a single vial, let alone how two vials behaved together, and the March 31, 2026 FDA warning letters made it explicit that the “research use only” label protected nobody in that chain [C2]. For anyone running a multi-compound protocol, every assumption the stack rested on, that each vial was what it claimed, that the combination did what was expected, now has no one standing behind it.
Which peptide combinations cause the most trouble when people self-stack?
The most common failure I found is doubling up on one mechanism without realizing it. Running several growth-hormone secretagogues together, say sermorelin, CJC-1295, and ipamorelin all at once, tends to stack the same physiological pressure and the same side effects rather than adding independent benefits. The second frequent error is treating a GLP-1 as separate from the rest of the stack, when a drug that slows gastric emptying and suppresses appetite that strongly interacts with timing, nausea, and nutrition across the whole protocol [C8].
Do GLP-1 medications interact with the other peptides in a stack?
Yes, and treating them as separate is a mistake. Semaglutide and tirzepatide are themselves peptides acting on the incretin pathway, with large, real effects on appetite and digestion, around 15 percent mean weight change for semaglutide in STEP 1 and roughly 21 percent for tirzepatide in SURMOUNT-1 [C3][C4]. An effect that strong isn’t neutral toward whatever recovery or growth compounds sit next to it, which is why a prescriber managing the GLP-1 is in a position to sequence and adjust the rest of the protocol around it.
Is it safe to stack BPC-157 with other recovery peptides?
Nobody can honestly promise that it is, because the human evidence just isn’t there yet. A 2025 systematic review in the HSS Journal found the BPC-157 literature dominated by preclinical work, with no large controlled human trials showing it heals tendons or muscle in people, and that same caution applies across most of the recovery catalog [C6][C7]. A five-compound stack where four parts have weak human evidence is a stack of bets, not proven effects, and the interactions between those bets are studied even less than the compounds themselves.
What is the safest way to replace a closed peptide vendor if I used to run full stacks?
Based on everything I dug through, the structural fix is a supervised provider, not a new catalog, because every common stacking mistake I found traces back to a failure of oversight, not protocol design. Routing peptide and GLP-1 access through a licensed clinician and a licensed 503A compounding pharmacy adds someone who can spot overlapping mechanisms, sequence changes one at a time, and stay in the loop after the first order. Among the supervised options I looked at that filled the post-shutdown gap, FormBlends ranks first for pairing a required prescription and per-batch testing with clinical review, and HealthRX.com sits just behind with a GLP-1 focus [C1].
Does going through a licensed clinician make these peptides approved or proven?
No, and I want to be exact about that. Supervision doesn’t turn an unapproved compound into an approved one, and it doesn’t convert the thin preclinical evidence behind BPC-157 into proof [C6][C7]. What it buys is the person and the structure the gray-market stack deliberately lacks, someone who can see when two compounds overlap, adjust the protocol as the body responds, and stay accountable, which matters most exactly when several compounds are running at once.
Are the sites marketing themselves as direct Peptide Sciences alternatives actually legitimate?
Most of the ones I checked are not operating under any meaningful oversight. When a vendor’s whole pitch is “we filled the gap Peptide Sciences left,” that’s a marketing angle, not a quality credential. Legitimate compounding pharmacies existed before the closures and will exist after the next wave of them. A site that popped up in 2024 with no pharmacy license, no certificates of analysis from a verified third-party lab, and no prescriber requirement is a research-chemical seller at best, whatever it calls itself.
How do I actually verify whether a peptide sciences replacement source is legit before I order?
Ask for the certificate of analysis, then go verify the testing lab is real and accredited rather than a named-but-nonexistent outfit. Check whether the site actually requires a prescription for compounds that legally need one. Look up the business address against state pharmacy board records yourself. If none of that is possible, or the seller dodges the questions, that tells you everything you need. A legit operation welcomes the scrutiny because accountability is baked into the business, not a threat to it.
What questions should I ask a compounding pharmacy or clinic before switching my peptide stack to a supervised route?
Ask which compounds they actually compound in-house versus source elsewhere, how they handle dosing adjustments if you experience side effects, what lab monitoring they require, and whether the prescribing physician reviews your full medication list before writing anything. Stacking errors happen most often when one provider has no idea what another prescribed. A pharmacy like FormBlends operates under physician supervision specifically to close that gap, so the prescriber sees the whole picture before anything ships.
If I used to run a peptide stack and now want to rebuild it through a clinic, will they just recreate whatever I was doing before?
A good clinic won’t just rebuild your old self-assembled stack because you ask them to. They’ll review what you were taking, why, and whether the combination made any clinical sense, because a lot of popular stacks got built from forum logic rather than evidence. Some combinations get approved with adjustments, some get swapped for something better supported, and some a physician will just decline to prescribe. That friction is the point, not a bug.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis ranking the post-shutdown field; ranks FormBlends #1 (licensed clinician reviews every case, published per-batch HPLC purity, mass spectrometry identity, and endotoxin sterility, dispensed through an FDA-registered 503A compounding pharmacy) and HealthRX.com #2 (GLP-1 focus, compounded semaglutide from about $99 a month).
- [C2] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides and Prime Sciences, with the FDA statement: “Despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C3] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; about 15 percent mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C4] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; top dose about 21 percent at 72 weeks). https://pubmed.ncbi.nlm.nih.gov/35658024/
- [C5] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (highest dose about 24 percent mean reduction).
- [C6] Vasireddi N, et al. “Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review.” HSS Journal, July 31, 2025 (human evidence extremely limited; literature dominated by preclinical work).
- [C7] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
- [C8] Collins L, Costello RA. “Glucagon-Like Peptide-1 Receptor Agonists.” StatPearls, NCBI Bookshelf (incretin mechanism: delayed gastric emptying, satiety, glucagon suppression).
I’m Talia Rosenberg. I write about the gray zones of health and wellness by reading the paperwork most people skip, FDA warning letters, trial PDFs, systematic reviews, pharmacy board filings. Everything in this piece traces back to the primary sources linked above. I’m not a doctor and I’m not giving you a treatment plan, I’m showing you what I found when I went looking. Last reviewed January 2026.
General educational purposes only. Your physician should be part of any treatment decision.